Dropped object fell from crane – Poor communication/lack of awareness/control of work
A member has reported a dropped object incident in which a CCTV camera (weighing 5.8kg) fell approximately 3m down a crane pedestal ladder before being arrested by its data cable, which prevented it falling on to the main deck. A 50Te crane was tasked with the recovery of subsea equipment. During this operation the crane was started and rotated outboard portside in order to deploy the hook to seabed.
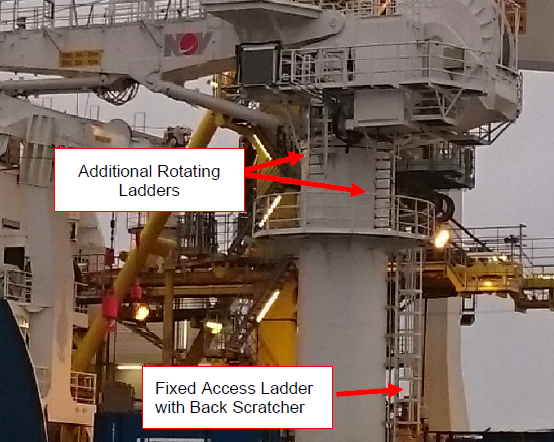
This 50Te crane was designed with a fixed access ladder, complete with a ‘backscratcher’ from the main deck to the first level walkway on the crane pedestal, a height of 7.4 meters. From this walkway, there are three additional ladders fixed to the crane, two of which are for maintenance purposes and the other leads to the crane operators control cabin. These additional ladders rotate with the crane as it is slews in the required direction.
As the crane was rotated, one of these ladders caught the CCTV camera that had been secured to the walkway following maintenance during the previous shift, pulling it approximately 1 meter to the access hatch, where it fell before being arrested by the data cable.


Our member’s investigation noted the following:
- The CCTV camera had been removed from its mountings the day before the incident to allow investigation of reports that it was not working properly;
- The faulty camera could not be repaired at the time and as such, was secured to the crane walkway using tie-wraps;
- The access hatch located on the walkway was left in an open position while crane operations were ongoing. This is common practice and is done to allow suitable access/ogress to and from the crane in the event of a crane breakdown or if a rescue operation is required. The crane design prevents the hatch from being opened when one of three ladders are positioned over it, restricting access/egress;
- The work conducted on the camera and the status in which it was left was not communicated to the crane operator or the project construction crew at shift handover/TBT. The on-shift crane operator was not made aware that work had been conducted on the crane pedestal and did not identify the CCTV camera during the pre-use inspection;
- The CCTV repair was considered to be covered under a company ‘routine’ duty for work on low voltage systems;
- The correct process for approving ‘routine’ duties’ had not been followed which resulted in this particular ‘routine’ duty being absent from the appropriate register of such duties kept on the vessel.
Lessons learnt, actions taken, and conclusions:
- There was a lack of awareness and risk perception of the hazard presented by the rotating ladders;
- A more thorough pre-use inspection of the walkway would have discovered the potential dropped object;
- Improved communication – particularly at shift handover – between all parties would have raised awareness of the operation;
- Had this operation been conducted under a permit to work (PTW) or the correct process followed for ‘routine’ duty activities, awareness of the operation would have been greater. It is important to highlight that control measures had been implemented by those conducting the work to ensure safe execution of the task and that these were removed when the worksite had been deemed safe;
- Personnel were clear of the crane pedestal at the time of the incident due to the task being conducted and the member’s procedures for controlling access to the crane when in use. Our member reviewed processes for controlling access to ensure they were robust in protecting personnel from injury. The safe system of work for all ladders on worksites, both permanent and temporary was reviewed, with consideration being given to suitability of design, position and access/egress.
Members may wish to refer to the following incident (search word: crane):
- Near-miss: Personnel almost caught between crane house and scaffold pipe – In this rotating crane incident, a direct cause was failure to communicate -the crane operator was not informed at the start of the work. Also, a ‘last minute risk assessment’ by the non-destructive examination (NDE) inspector did not reveal the actual risks, there was inadequate initial instruction, and information was not communicated properly to all the involved parties. The TBT process was not conducted in accordance with established procedures and the work process was discussed without involvement of all parties (deck crew/crane operator).
Safety Event
Published: 13 September 2016
Download: ![]() IMCA SF 23/16
IMCA SF 23/16
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.