Lost time injury (LTI): leg injured while dealing with vent flaps
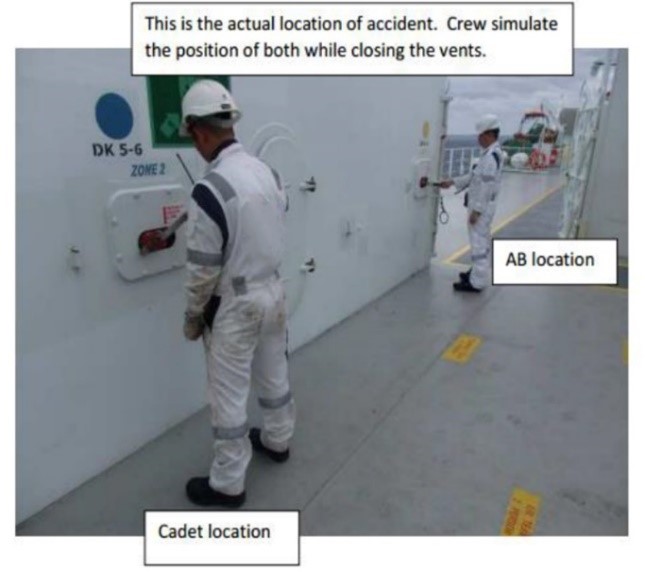
A member has reported an incident in which a crew member suffered a serious leg injury whilst closing ventilation flaps. Two crewmen, one an AB, the other a more inexperienced Cadet, were on the upper deck closing the flaps when a crank handle used to wind the flaps closed became detached and flew through the air. It hit one of the crewmen on his right shin, lacerating his skin and fracturing his leg. He was evacuated by helicopter for treatment ashore.

Our members’ investigation noted the following:
- Each crewman closed a different vent, winding the handles anti-clockwise;
- The Cadet felt no more counter weight on his crank handle and informed the AB that his vent was closed;
- The AB told him keep turning the handle to “make sure”:
- by continuing to turn the handle counter clockwise the cadet had started to raise the vent flap again (turning the cable the opposite way onto the drum);
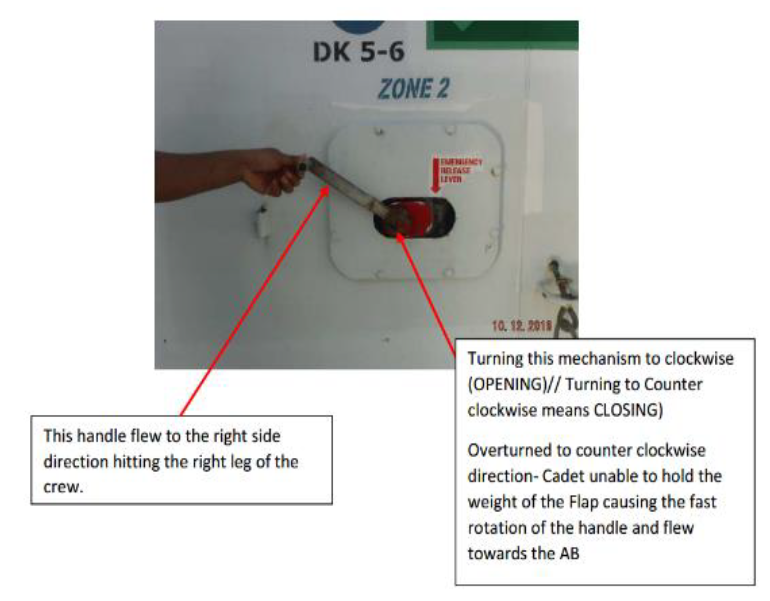
- After less than a minute of further turning the cadet felt weight coming onto the handle again and accidently let go. The handle quickly rotated clockwise and the crank handle detached and flew through the air, hitting the AB;
- The vent house door remained padlocked following a port call – there was no visual means of checking that the flaps were closing;
- There was no written Risk Assessment for the operation;
- There were a number of immediate causes:
- the emergency release lever was in the wrong position
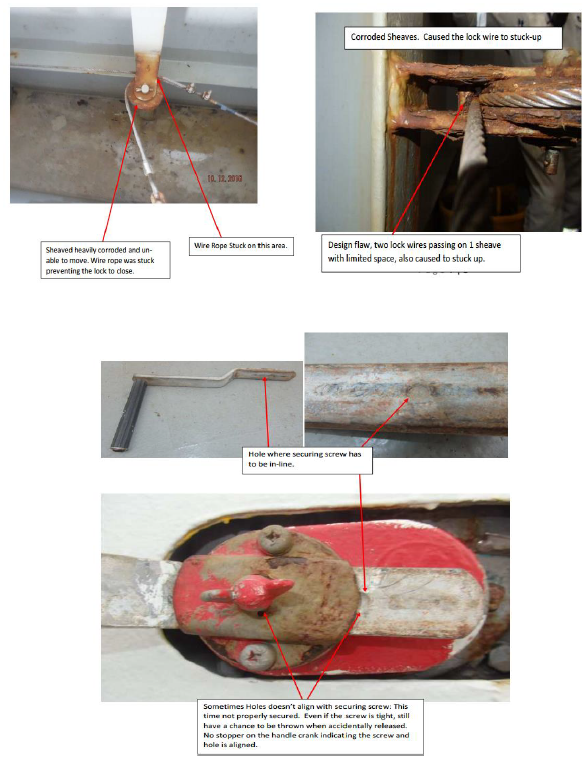
- the safety locks were stuck open due to a rusted sheave trapping the wires
- the shallow indentation and wingnut screw used to secure the handle was inadequate;
- Causal factors that were identified:
- lack of experience and knowledge: The Cadet did not trust his initial judgment that the flap was closed and followed the instruction to keep turning. A more experience crewmember may have been more confident to trust his instinct. He was not aware of proper position of the emergency release and was confused by the instructions painted above
- inadequate planning and procedures, inadequate maintenance and design of equipment;
- Root causes identified:
- risk was not fully assessed or understood and was considered tolerable
- instructions and warnings were unclear and confusing
- maintenance of the wires, sheaves, winches locks and handles was not adequate
- the securing mechanism for the crank handle was poor and left the handle inadequately secured;
- The preventative action taken was to:
- prepare training in this operation
- develop a risk assessment including minimum crewing required to do the task safely
- appropriate maintenance and repair of the wires, sheaves, winches locks and handles
- Ensure instructions are correct.
Members may wish to refer to the following incidents:
Safety Event
Published: 12 April 2017
Download: ![]() IMCA SF 08/17
IMCA SF 08/17
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.