Fall from height during yard visit
What happened
A yard worker fell 4m from the main deck to a mezzanine deck. The injured worker suffered a compression fracture in his right ankle.
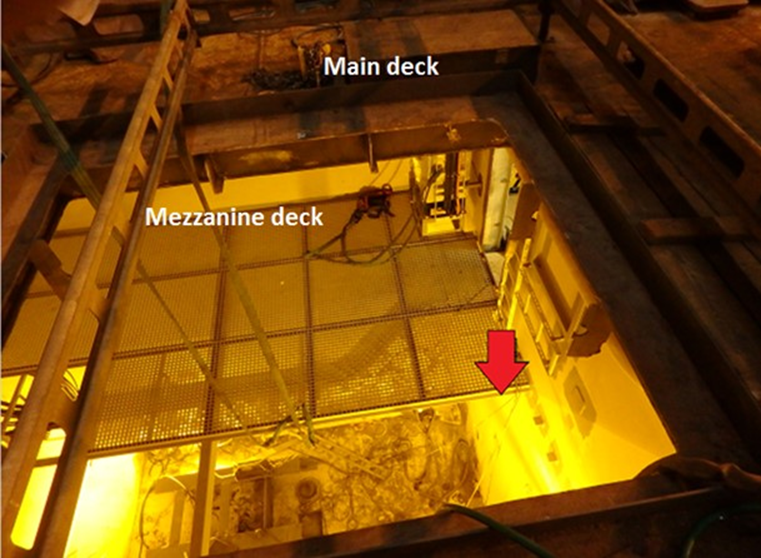
During a yard visit, pieces of grating were being manually lowered with a rope down through an opening on the main deck. The opening on the main deck was barred off by a scaffold. No fall protection was requested by the people on the main deck.
Two workers should have been on the main deck and two on the mezzanine deck. The workers on the mezzanine deck were wearing fall protection. However, at the time of the incident there were three workers on the main deck, and one worker on the mezzanine deck.
A piece of grating got stuck on an edge on the main deck. This was observed by a co-worker who happened to be nearby. He intervened in the work operation. The workers on deck shifted the grating about 15 centimetres. As the grating shifted, the new worker continued to hold onto it, lost his balance and fell.
The injured worker was a part of the scaffolding team but was not a part of this planned operation. He decided to help his co-worker. He was wearing a fall arrester but did not clip into an anchor point.
What went wrong?
- Attitude and behaviour – the injured person and the work team showed lack of safety awareness;
- Non-compliance with personal protective equipment (PPE) – the injured worker was wearing a fall arrester but didn’t clip on to an anchor point. Also, whilst the gratings were usually handled manually, there were taglines attached, but these were not used;
- Competence and experience – the injured worker had worked as a scaffolder at the yard for years, had experience and training in scaffolding and working at height, and possessed competence certification. All the work team including the injured person were experienced in working at height;
- Language – the injured worker spoke neither English nor Norwegian. Translation was conducted by co-workers. This yard routinely employs foreign workers with limited or no skill in English, although laying down rules for sub-contractors on how such workers were to be deployed;
- Teamwork/communication – the investigation team has not been able to conclude if the worker was asked to support, or if he intervened on his own initiative. Different versions of the story have been raised in interviews;
- Management and supervision – the work team was wrongly organised. There were four workers in the work team, there were supposed to be two workers on the main deck and two workers on the mezzanine deck for this operation. At the time of the incident there were three workers on the main deck, and only one worker on the mezzanine deck;
- Safety systems – a Permit to Work and Toolbox Talk had been conducted, and the injured person had been a part of the toolbox talk (see earlier remark about language). The foreman for this work considered it to be known to the work team, so no specific job safety analysis took place, and there was insufficient focus on the shipyards’ “We Care” safety campaign, as supervisors and co-workers did not pay attention to the injured person not using appropriate working at height equipment.
What were the causes?
- Immediate cause: the injured worker rushed into a work situation he was not supposed to be a part of. He did not consider the risk in the operation and did not secure his fall arrest to an anchor point;
- Underlying causes of the Incident: the injured worker did not comply with working at height standards and did not pay attention to the risks in the work situation;
- Root Causes: the investigation concluded that these were weaknesses in safety awareness and management of work in the actual situation.
What lessons were learnt?
- Ensure closer follow up of yard to ensure compliance to safety awareness;
Executive (high level) commitment to safety is paramount for building a strong safety culture – particularly when multiple organizations are working together in a shipyard.
Members may wish to review Guidance on safety in shipyards.
Members may also wish to review the following incidents:
Safety Event
Published: 13 July 2017
Download: ![]() IMCA SF 17/17
IMCA SF 17/17
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.