Dropped object: dislodged flex-joint laydown tool component
What happened?
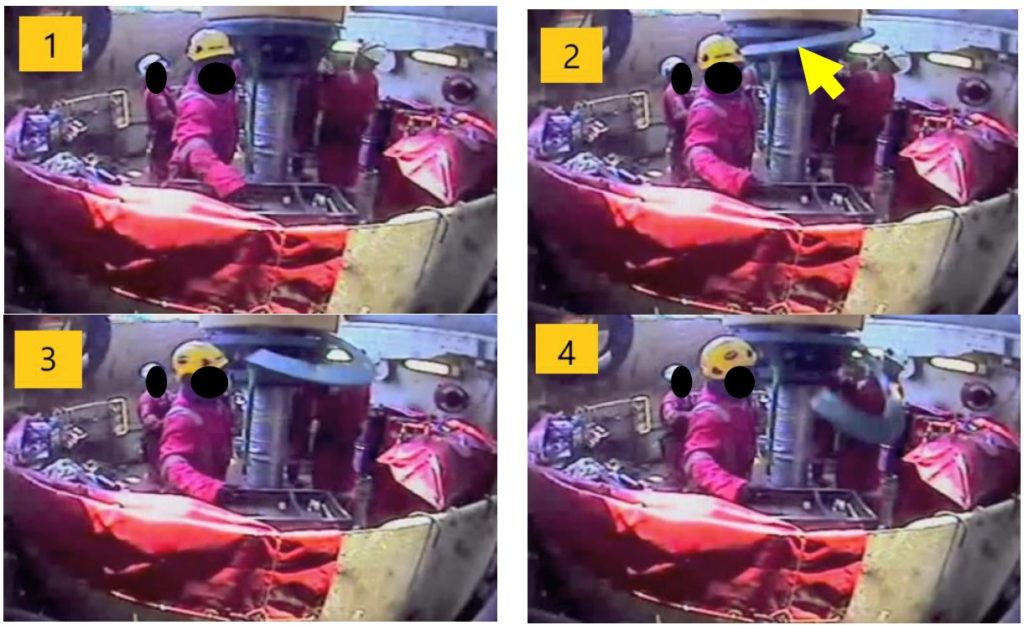
During removal of the anti-rotation/laydown tool from a Flex-Joint, a load-ring half plate, weighing 85kg, was inadvertently dislodged and dropped about 1.8m to deck.
Crew on a J-Lay Tower were removing the anti-rotation device/laydown. The tower was tilted to 5 degrees at the time of the incident. A team of riggers and technicians proceeded to remove the half plates, which form part of the laydown tool. After the load ring securing plate was removed and the final jacking bolt had been loosened, one load ring element slid out of the assembly and dropped down onto deck.
There were two persons closed to the dropped half ring. No one was injured during the incident.
What went wrong?
- Procedures not followed:
- The removal of the load ring plates did not follow the approved procedure. The task plan included the manufacturer’s procedure which described the correct way to do it, which required eye bolts and rigging to remove the section of the laydown tool using a crane;
- The task of removing the load ring half plates manually/by hand was deemed to be faster and required less steps than the approved procedure;
- The risk associated with the removal of the heavy load rings by hand instead of using a crane was not assessed.
Actions
- Follow the instructions; keep to the procedures!!
- Any planned changes to the task plan or procedure should require a Management of Change process to be conducted to assess the risks from the change, apply the appropriate controls and gain authorization to proceed;
- If unsure of the correct method to execute a task, or the associated risks, personnel should always speak to their supervisor before attempting the task – don’t be afraid to STOP THE JOB.
Members may wish to refer to:
- Rope under tension parted on deck [“did not follow the company approved rigging arrangement”]
- High potential near miss dropped object [“task plan was not properly followed on site before conducting the operation”]
- Dropped wooden block in conductor support frame [“Procedures had not been updated to include” changes in practice; “Management of change (MoC) was not implemented/followed”]
Safety Event
Published: 25 November 2021
Download: ![]() IMCA SF 32/21
IMCA SF 32/21
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.