MAIB: Blockage of fixed CO2 fire extinguishing system pilot hoses
The UK Marine Accident Investigation Branch (MAIB) has published Safety Bulletin 1/2022 into a fire on board a roll-on/roll-off cargo ship in September 2021.
What happened
A fire broke out in the auxiliary engine room on board a roll-on/roll-off cargo ship. In an attempt to extinguish the fire, the ship’s crew activated the machinery space’s carbon dioxide (CO2) fire extinguishing system, but only half of the system’s gas cylinders opened.
What went wrong
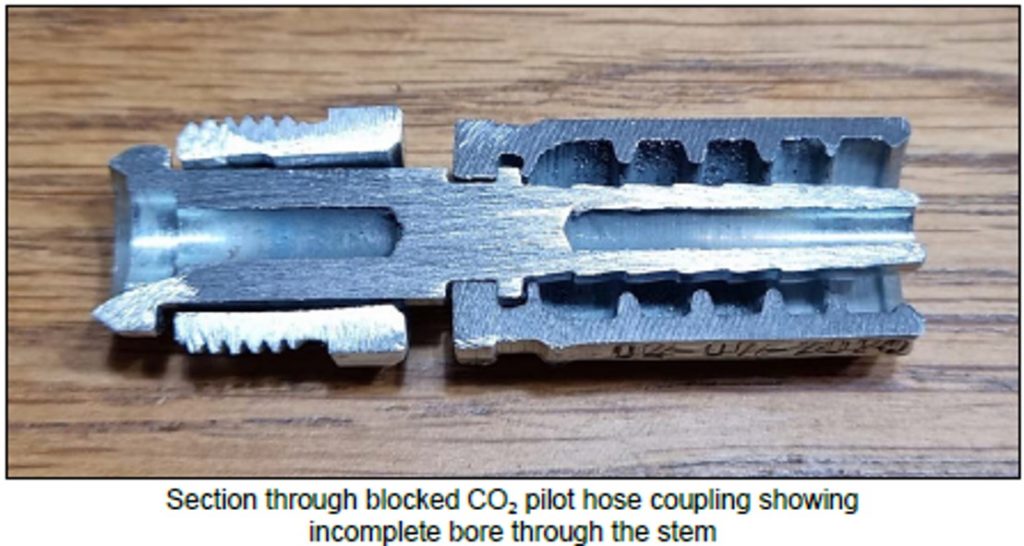
Investigation identified that one of the auxiliary engine room’s CO2 system pilot hoses was completely blocked. Subsequent examination and testing of the vessel’s fixed fire extinguishing systems identified two other similarly blocked hoses. It was discovered that the pilot hose couplings had not been fully bored through during the manufacturing process. The testing process also identified several coupling leaks in the pilot lines.
In March 2021, the pilot hoses had been replaced during a routine servicing by a fire safety company. Tests carried out at that time did not identify any faults with the system. Following the accident, tests were made of the high-pressure CO2 fire extinguishing systems on board the other vessels in the company’s fleet. These tests identified two similar pilot hoses that were blocked on one ship.
All the affected hose assemblies had been supplied to the fire safety company by one supplier. The hose assemblies had been produced under the terms of the classification society type approval held by that one supplier. Although the type approval required each completed hose assembly to be pressure tested, there was no specific test that gas could pass freely through the hose assemblies.
The hose used in the assemblies was provided in accordance with the type approval held by that one supplier, but that supplier had purchased the couplings from another hydraulics supplier, who in turn had sourced the couplings from a different manufacturer.
Lessons learned
- Ensure that crews are fully acquainted with the procedures for the manual activation of CO2 fire extinguishing systems in the event of the pilot actuation system failing;
- The fire safety company did not identify that some of the hose assemblies were blocked and that there were leaks in the CO2 system pilot lines;
- Neither the suppliers’ quality assurance processes, nor onboard installation testing processes, identified that the hose couplings had not been fully bored through;
- Amended procedures to incorporate a pneumatic flow test of the complete hose assemblies to verify that they are not blocked.
Members may wish to refer to:
- Firefighting (FiFi) Tank Outlet Blockage [a small mechanism was redesigned to eliminate a potentially life-threatening flaw]
- Faulty governors [pieces of a broken valve were carried in the hydraulic system. This caused malfunction of the hydraulic valve.]
Safety Event
Published: 21 April 2022
Download: ![]() IMCA SF 10/22
IMCA SF 10/22
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.