Lift bag near miss
What happened
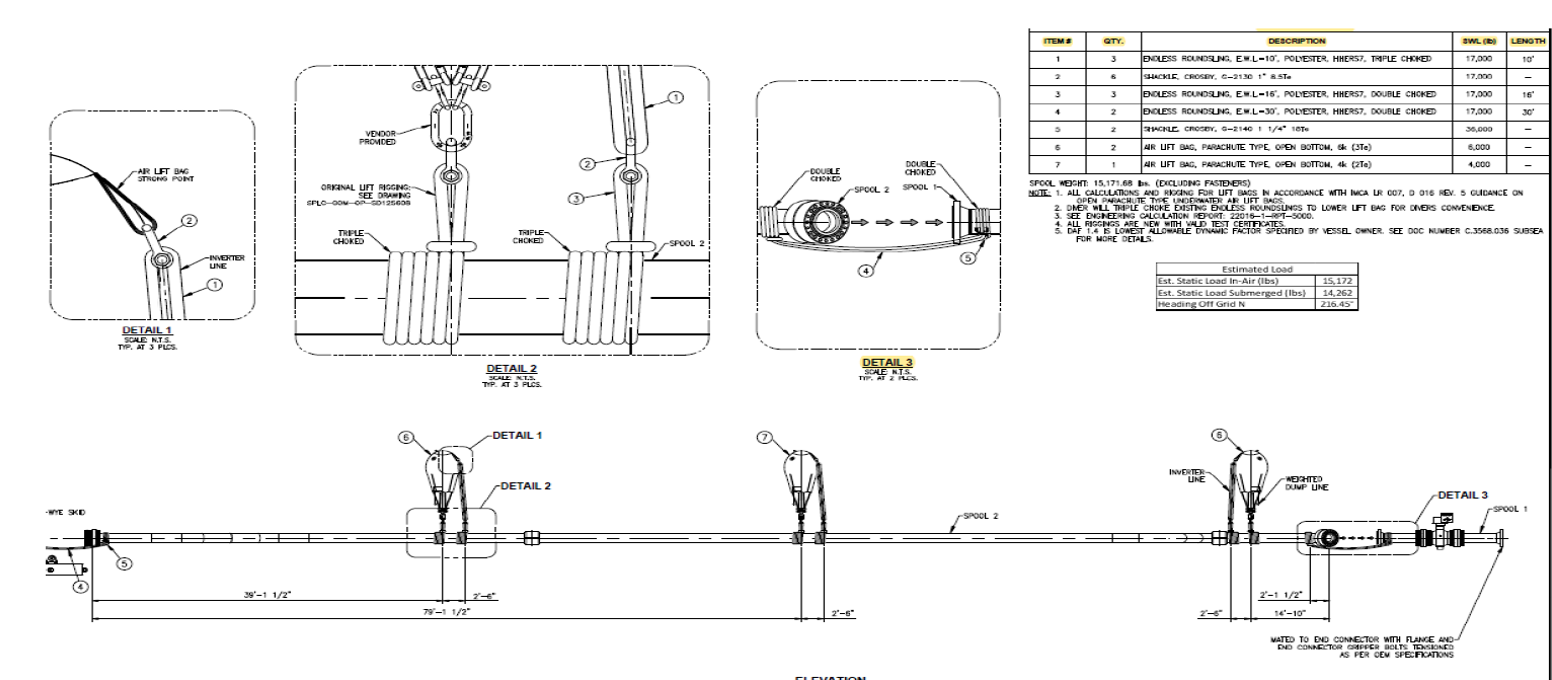
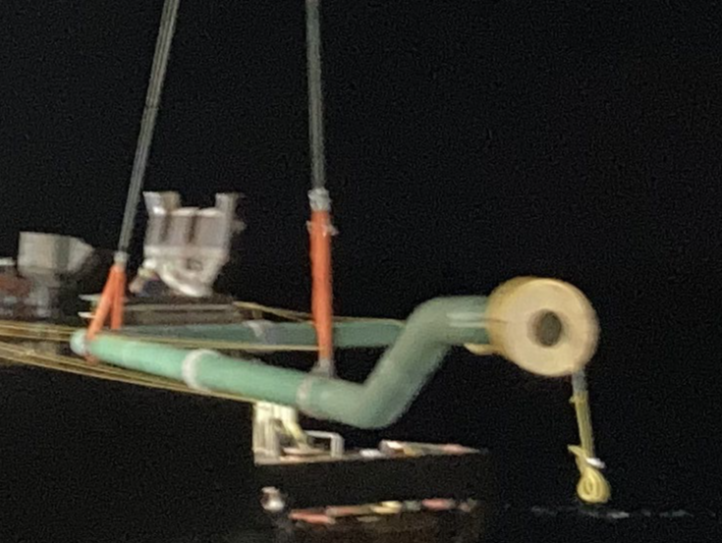
During the over-boarding of a spool, a lift bag while being inflated, ascended through the engineered rigging arrangement and was caught by the contingency rigging. The diver had rigged the lift bag inappropriately for the conditions. The lift bag was hooked into one eye of the sling, the sling then slipped out as the lift bag became inflated and was inverted with the safety strap. Our member considered this incident to have had the potential for a serious injury or fatality.
What went wrong
- Assumptions were made by the diver and by the supervisor, about the rigging, perhaps owing to:
- Poor visibility;
- Diver inexperience with lift bag operations;
- Complacency.
- The rigging arrangements were not correct nor verified as per procedure:
- Spool rigging and local in-field adjustment began to happen without proper documentation or formal management of change (MoC);
- The divers were multi-tasking, working in different locations on different concurrent tasks, and communications between the divers and diver supervisor were complex and unclear;
- The rigging had been changed earlier but this change had not been communicated to the dive team;
- As the final spool was lowered, late at night, rigging changes were not noticed.
- Existing procedures were not specific to this task:
- A 4-ton lift bag was identified in the procedure but was not available;
- The inverter rigging was not one size fit all, as the bags were different sizes, thus creating a scenario where diver rigging was required to lengthen or shorten the existing rigging;
- There were changes of personnel during the job:
- Superintendents were changed out;
- The bell run was split such that the diver that de-rigged the spool was not the same diver as inflated the lift bag that came loose.
- During the job, a finger incident occurred on the bell clump basket, and there was a safety stand down.

Lessons learned
- Ensure one single person is accountable for rigging, reporting to the Superintendent and collaborating with the dive team;
- Improve management and installation of rigging configurations;
- Ensure written procedures are not generic, are up to date, and reflect the details of the task in hand;
- Minimise multitasking to eliminate distractions and fatigue;
- Be additionally vigilant and ensure there is thorough communication:
- At crew change and at shift change;
- Between shore-side or yard and vessel;
- Between crew of different departments – dive, deck, bridge, project, etc.
Members may wish to refer to
Safety Event
Published: 13 March 2023
Download: ![]() IMCA SF 07/23
IMCA SF 07/23
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.