Fatality during lifting operations
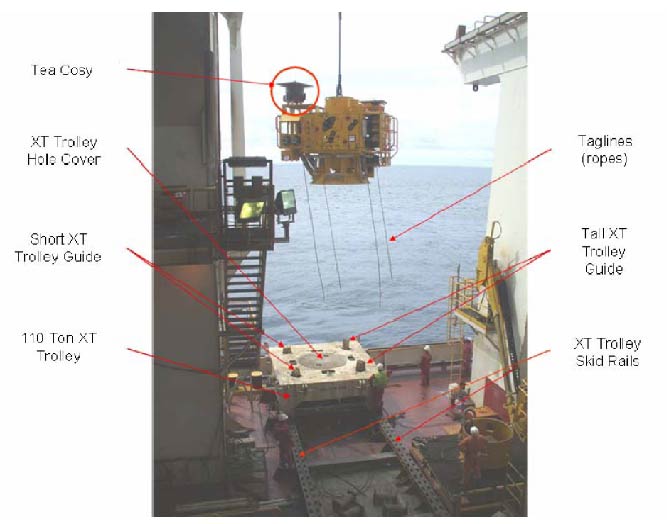
A member has reported an incident in which a fatality occurred during lifting operations. The incident occurred on a drillship while attempting to land a christmas tree (XT), using one of the vessel cranes, on to the XT trolley (see general view below). It was important to centralise the XT, which weighed 50 tons in air, on to the trolley.
Centralising guides were in place on the trolley but lifting conditions (heavy load, near vertical crane boom position and movements of floating unit) required significant planning and supervision for this operation.
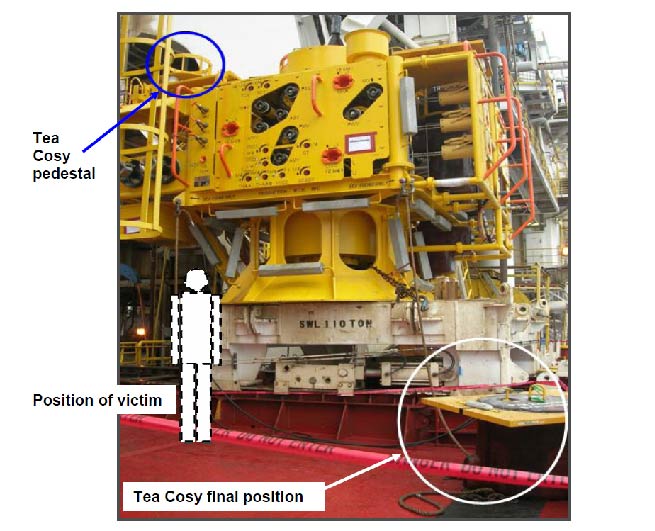
The tree was approximately 0.6m above the trolley for final positioning when the main hoist hydraulic motor of the crane failed catastrophically. The 50 ton XT fell on to the trolley and as a result a further item known as the ‘tea cosy’, weighing 335 kg, came loose from its pedestal on top of the XT and bounced off the XT on its way down to the deck. A member of the crew supervising the operation was struck by the tea cosy and died instantly.
Following investigation, the main causes of the incident were identified as follows:
- Failure in crane control:
- A week before the accident the main hoist hydraulic motor was replaced by an incorrectly sized motor available onboard the vessel. Though both motors look very similar and can be installed in the same position they have very different torque characteristics and are designed for different purposes
- There was no in-depth investigation performed following the first hydraulic motor failure a week before
- The hydraulic motor was changed without reference to the crane manufacturer’s manuals (which were available onboard)
- A review of the preventive maintenance system used onboard identified defects in spare traceability, maintenance plans and personnel competency and training;
- Failures in operational control:
- The tea cosy was not fully secured on its pedestal. Under ‘normal’ lifting conditions, full securing of the tea cosy was not considered necessary; the sudden shock due to the free fall of the entire XT had not been identified as a hazard
- Free fall of XT assembly was not considered in the risk assessment
- The victim was standing adjacent to the XT during the final landing; though he was co-ordinating the operation he had not been involved in the pre-job meeting.
The following recommendations and corrective actions were proposed:
- Ensure all are aware of the possibility of inappropriate hydraulic motors interchange on crane SEATRAK Model 7228;
- Ensure full assessment during lifting/crane audits of onboard preventive maintenance system;
- Improve thoroughness of risk assessments in order to correctly identify all hazards. Results and findings must be communicated during pre-job meetings to all persons involved in operation;
- The design process and hazard identification study (HAZID) review of the XT should not only focus on final use of the product but also upon packaging, fastening, lifting, transportation and installation conditions and hazards. This should include design of the tea cosy pedestal and fastening method of all non permanently attached items;
- Redesign and re-engineering of the centralising guides on the XT trolley;
- More careful attention to the handling of heavy lifts on a drillship with a near vertical crane boom.
Safety Event
Published: 6 May 2009
Download: ![]() IMCA SF 06/09
IMCA SF 06/09
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.