Diver injured during subsea lifting operations
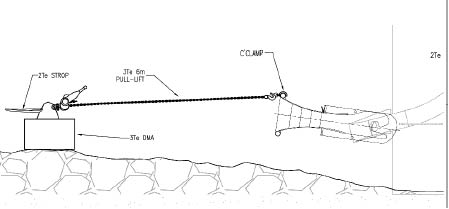
A member has reported an incident in which a diver was struck and injured by a two tonne weight as it was being deployed from the vessel crane during subsea installation work. The incident occurred when two divers were assisting in the installation of an external bell mouth on to its protruding J-tube mounting points at an offshore wind turbine base pile in 23 metres of water. Shortly after the start of the dive it was decided to send down a two tonne dead man anchor (DMA) and a lever hoist. These were required to pull the bell mouth into the correct alignment for fitting. Before the DMA was deployed, the diving supervisor instructed both divers to move in a specific direction to a safe location away from the bell mouth. The divers were also told to look upwards to observe the DMA deployment. Diver 1 initially followed these instructions but he later moved back into the danger zone without direction from the supervisor. Diver 1 was subsequently struck by the DMA as it was lowered by the vessel crane from the surface. Diver 1may also have been pinned to the seabed by the weight of the anchor for a few seconds until it was lifted off him by the crane. The injured diver was treated on-board the vessel and subsequently evacuated to hospital by helicopter. The diver was released from the hospital later the same day and sent home on temporary sick leave.
The incident demonstrates that divers keen to complete their work may be tempted to move into danger zones during the course of subsea lifting operations.

Our member’s investigation revealed the following:
- Immediate causes:
- Lack of knowledge of the whereabouts and depth of the subsea load during its deployment through the water column;
- Over-rapid lowering of the load;
- The subsea load was lowered all the way to the seabed with no appropriate mid-water stop point;
- The diver was directly below the load as it was being lowered;
- Poor communication and co-operation between the diving supervisor and the divers;
- Owing to misunderstanding, diver 1 failed to follow the instructions of the diving supervisor;
- The diving supervisor failed to realise or notice that the diver had moved back into the danger zone.
- Root causes:
- Inadequate hazard identification and risk assessment;
- No common toolbox talk held before the start of the operation;
- No lift plan or safe working procedure for deploying the load whilst divers were in the water;
- Reliance on the diver following instructions; failure to take sufficient account of human factors leading to errors (mistakes and violations);
- Complacency – the operation was perceived as being a simple, familiar and repetitive task, and personnel may have been operating within a ‘comfort zone’.
Our member drew the following lessons from the incident:
- All personnel (including divers) should attend toolbox talks to review the plan before the start of subsea lifting operations;
- Appropriate risk assessment should take place to cover the particular challenges of vessel lifting operations in support of diving operations;
- Lift plans prepared by competent persons should be in place before the start of subsea lifting operations;
- Ensure effective communications between all members of the lifting team;
- Personnel (including divers) should never work underneath loads;
- Divers should retreat to confirmed safe locations (e.g. the dive basket or bell clump weight) during the lowering or lifting of loads through the water column and remain there until they are alerted that the chosen stop point has been reached;
- Use of travel length indicators to stop loads at an agreed distance above seabed;
- Use of specific lift deployment speeds in lift plans/procedures;
- Loads should be lowered in a controlled manner at specific and agreed speeds, rather than in free fall;
- Equipment and procedures should be in place to enable the crane driver and diving supervisor to know the depth of loads as they are lowered through the water column;
- Use of suitable stop points in the water column so that loads are not deployed straight to the seabed (or lifted straight to the surface), allowing time for divers to retreat to a safe location.
Members may wish to refer to the following IMCA documents:
Safety Event
Published: 11 October 2012
Download: ![]() IMCA SF 10/12
IMCA SF 10/12
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.