Fatal fall from height on-board Seatruck Pace in Liverpool in December 2018
What happened?
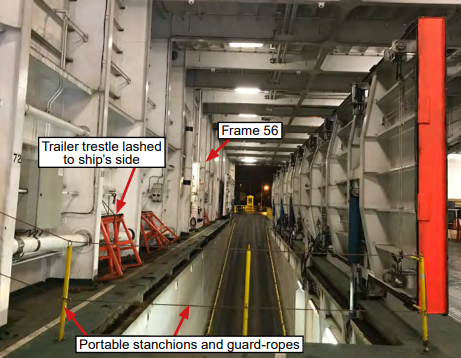
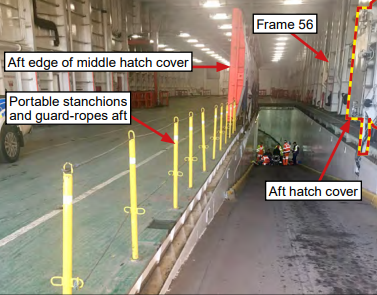
The UK Marine Accident Investigation Branch (MAIB) has published accident Investigation Report 9/19 into a fatal fall from height. A crewman from the Cypriot registered ro-ro freight vessel Seatruck Pace died as a result of 4.5 metres fall through a vehicle ramp hatch.
The crewman was working alone and preparing to paint the leading edge of the open ramp hatch cover. For reasons that could not be determined, the crewman crossed a temporary safety barrier guarding the edge of the open hatch and walked along a narrow deck edge between the ships side and the open hatch on which several trailer trestles were stowed. The crewman’s fall was not witnessed but it is evident that he had fallen at or about the same time as one of the trestles. He was treated at the scene before being taken to hospital. He died three days later.
What went wrong?
- The crewman crossed a safety barrier protecting an open hatch;
- Risk seen as tolerable – the risk of falling was accepted, having probably taken similar risks in the past;
- Work practices indicated that adherence to the vessel’s safety procedures was based on routine rather than of understanding and conviction.
What actions were taken?
The following actions were taken by the owners:
- Reminded Masters of the dangers of bypassing safety control measures and prompted them to review the safety of deck openings;
- Provided safety chains, fittings and warning signs for use on the temporary barriers rigged on the main vehicle decks of its ferries;
- Reviewed its risk assessment and permit to work (PTW) concerning working at height;
- Introduced a procedure for recording the use of safety harnesses;
- Committed to ensuring that all Masters and safety officers complete a Maritime and Coastguard Agency safety officers’ training course;
- Completed a ‘safety culture survey’ among its senior management, and senior managers have attended the Health and Safety Executive’s (HSE) ‘Behaviour Change – Achieving Health & Safety Culture Excellence‘;
- Engaged HSE consultants with the aim of forming a safety culture steering group and implementing the HSE’s ‘Safety Climate Tool’.
Members may wish to look at a number of other incidents where a causal factor was that risk was ‘seen as tolerable’: legacy.imca-int.com/alerts/search-safety-flash/?swpquery=tolerable.
Members may wish to refer to:
- Fatality: Fall from height in shipyard
- Fatality: fall from height
- Working at height (Be prepared to work safely, short video)
- Working at height (IMCA SEL 009, long video)
Safety Event
Published: 17 September 2019
Download: ![]() IMCA SF 22/19
IMCA SF 22/19
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.