Fatal incident during change-out of chain wheel (gypsy) on anchor handling tug supply (AHTS) vessel
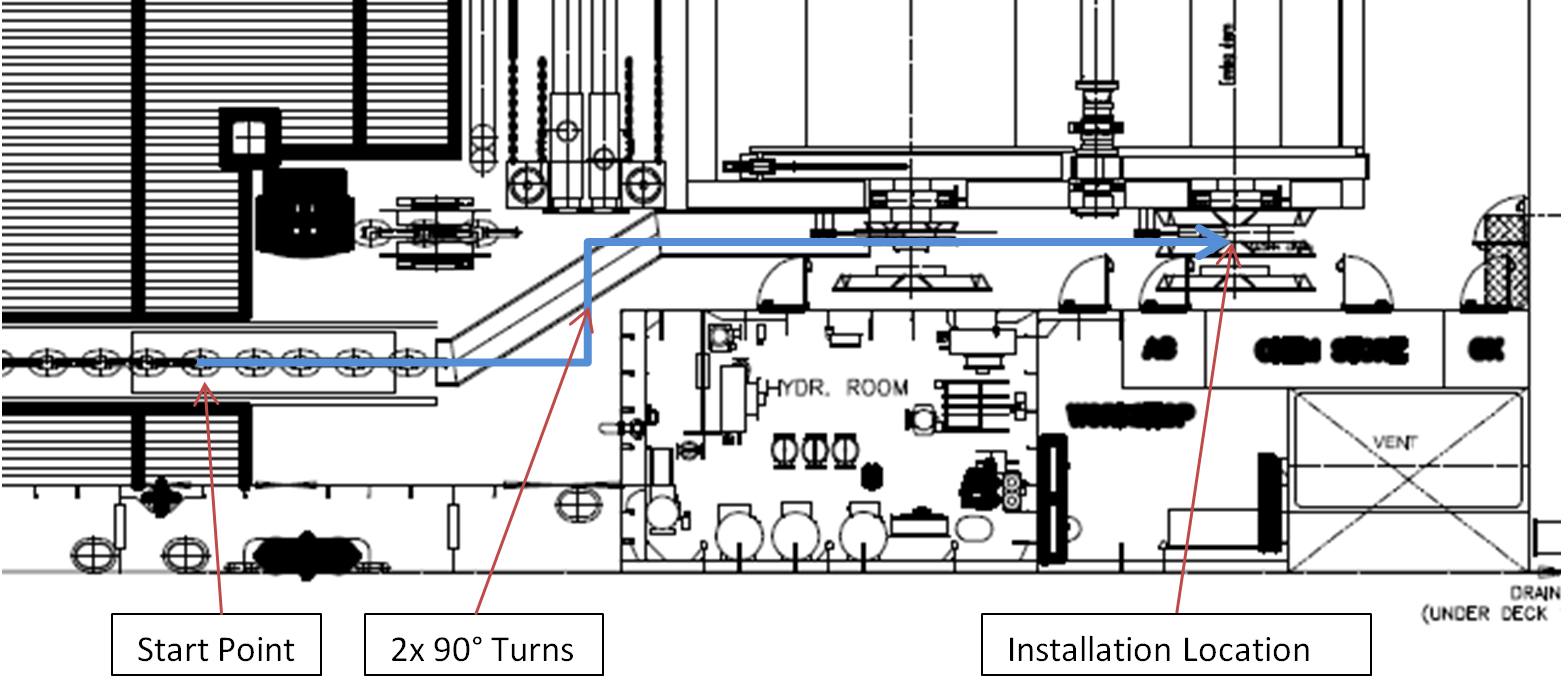
A member has reported an incident in which one crewman died and another received minor injuries when a gypsy wheel fell over whilst being moved, resulting in two crew members being trapped between it and a cargo rail bulwark. The incident occurred when a vessel was mobilising for a project which required the use of an 84mm wide gypsy wheel. At the time the starboard side forward winch was fitted with a 105mm unit. This was removed and stored on the main deck. Installation of the 84mm unit then started.
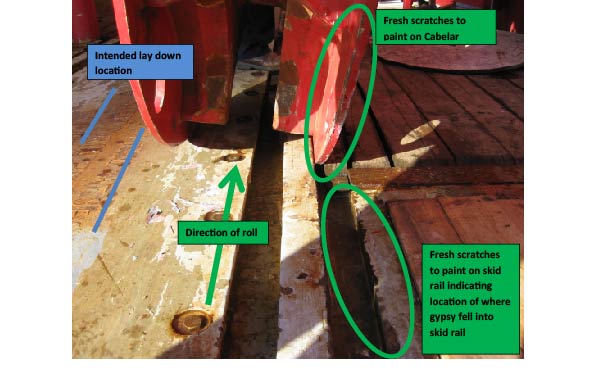
The crew disconnected the gypsy wheel from the crane without checking its final landing position. Therefore, they did not see that the rims of the gypsy wheel were on each side of the skid rail for the chain lifter. Immediately after disconnecting from the crane, the crew started to roll the gypsy wheel. This resulted in the starboard rim dropping into the gap in the rail causing the gypsy wheel to tip beyond balancing point. It fell over and pinned two crew members against the bulkhead. This resulted in one fatality and one first aid case.
Our member’s investigation noted the following:
- The immediate causes were:
- Gypsy wheel rolled into skid rail causing it to tip over
- Lack of risk management:
- Failure to identify hazards and risk
- Failure to comply with safe working practices;
- Contributing factors:
- Inadequate design review for this particular mode of operation conducted by vessel
- Insufficient lifting or handling appliances for handling and changing the gyps wheel;
- Root Causes:
- Inadequate monitoring and verification of organisational performance
- Weaknesses identified in the design review processes
- Lack of effective implementation of risk management.
The lessons drawn were as follows:
- Gypsy wheel should not be manually handled or rolled;
- Monitoring and verification of worksite performance was found to be inadequate.
The actions taken were as follows:
- Company-wide instruction forbidding free-rolling of these heavy items;
- Technical task force to evaluate a safe method for the installation of gypsy wheels in the short and long term and review change out methods across the fleet; . All vessels to review and re-risk assess current methods for handling gypsy wheels and submit risk assessment for approval.
Members may wish to refer to the following similar incidents (key words: crush, fatality):
- Crewman injured when steel plates fell against him
- Fatality: Man overboard (the crewman in this example fell overboard as a result of the sudden and unplanned movement of heavy objects)
- Fatality during lifting operations
Safety Event
Published: 2 April 2015
Download: ![]() IMCA SF 05/15
IMCA SF 05/15
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.