Lost time injury (LTI) during mooring operations
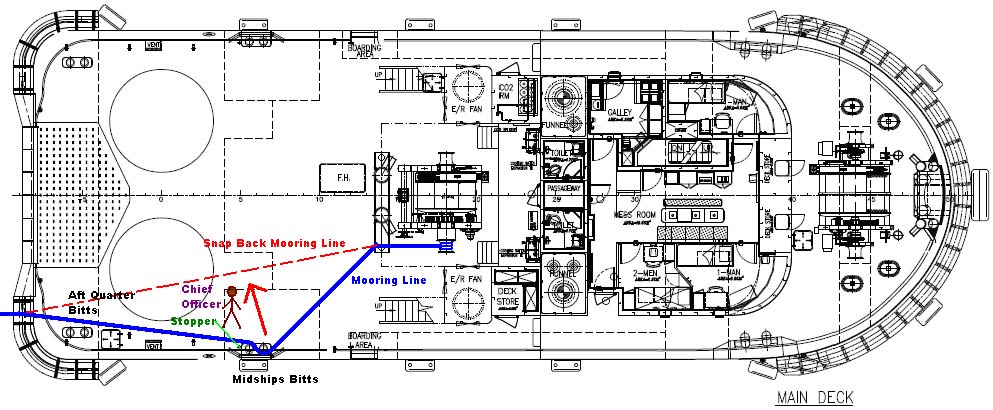
A member has reported an incident in which a crewman (the chief officer) suffered head injuries during mooring of a tug to a Single Buoy Mooring (SBM). The tug was mooring up to the SBM in order for the dive team to be able to complete ‘routine’ surface maintenance. Once the tug was in position it was realised that the vessel needed to move around 15 metres in order for the divers’ umbilical to reach the SBM. The configuration of the mooring equipment and arrangement being used required the injured person to enter a snap back zone in order to place a stopper on the mooring line, prior to securing it to the bitts.
As he was about to start stoppering off the line, the mooring line slipped off the bitt, striking him on the chest. This pushed him backwards and lifted him up, which resulted in him falling backwards and his head making contact with the deck. He sustained head injuries including a fractured skull. The incident was reported immediately, the vessel returned to port and the injured person was taken to hospital.

Our member’s investigation revealed that the causes of the incident were as follows:
- The mooring arrangement used required the Chief Officer to work in the snap back zone;
- The mooring arrangement used facilitated a vertical movement upwards (The midship bitts have a slight inboard inclination, the height difference between the mooring roller and midship bitts created an angle and the length of the horizontal extension arm is not long enough to present a sufficient safety guard);
- There was a deviation from normal operating procedure – inadequate MOC.
Our member took the following lessons to prevent recurrence:
- Reiterated importance of being able to STOP THE JOB in case of unsafe operations;
- Took steps to ensure crew were fully informed of risk and control measures;
- In cases where deviating from an agreed plan of operations, stop the job, re-assess and communicate the additional hazards and control measures via a toolbox meeting;
- Ensured all personnel involved in the activity or completing simultaneous operations take part in the toolbox meeting;
- Ensured personnel were trained and have sufficient experience and knowledge to carry out a task;
- Implement formal MOC process for changes/deviations to normal operating procedures and changes to design of the ship.
Members may wish to refer to the following similar incidents (key words: mooring, tension):
- Finger injury whilst casting off towing line
- Mooring incidents
- Crewman fatally injured during mooring operations
Members may wish to use IMCA’s safety promotional poster on mooring safety:
- Mooring safety (poster)
Safety Event
Published: 14 July 2014
Download: ![]() IMCA SF 12/14
IMCA SF 12/14
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.