Lost time injury (LTI): Serious foot injury
A member has reported an incident in which a rope access technician suffered a serious injury to one of his toes, leading to partial amputation. During J-lay pipeline operations, a malfunction was discovered in the locking pin designed to lock off the hang-off clamp (HOC). The pin would move down, but not up. Maintenance of the equipment was arranged. A crewman was assigned to clean the hang-off clamp using a water jet, and during this process he was supervised, from the deck level, by the Chief Engineer and 1st Engineer. When the cleaning was complete, he confirmed using hand signals to his supervisors that the job was complete.
The supervising team alerted the crewman that there would shortly be a test movement of the locking pin in order to test the functionality of the equipment. The supervising team alerted the crewman of the imminent movement of the pin, giving signals that he should move to a safer location. He confirmed visually that he had received this signal, but did not move, remaining with his foot on the pin. The 1st Engineer gave instructions via radio that the pin should be moved. Whilst moving, the pin squeezed the toe cap of the crewman’s boot, causing injuries leading to partial amputation of his right big toe.

An investigation identified the following causes:
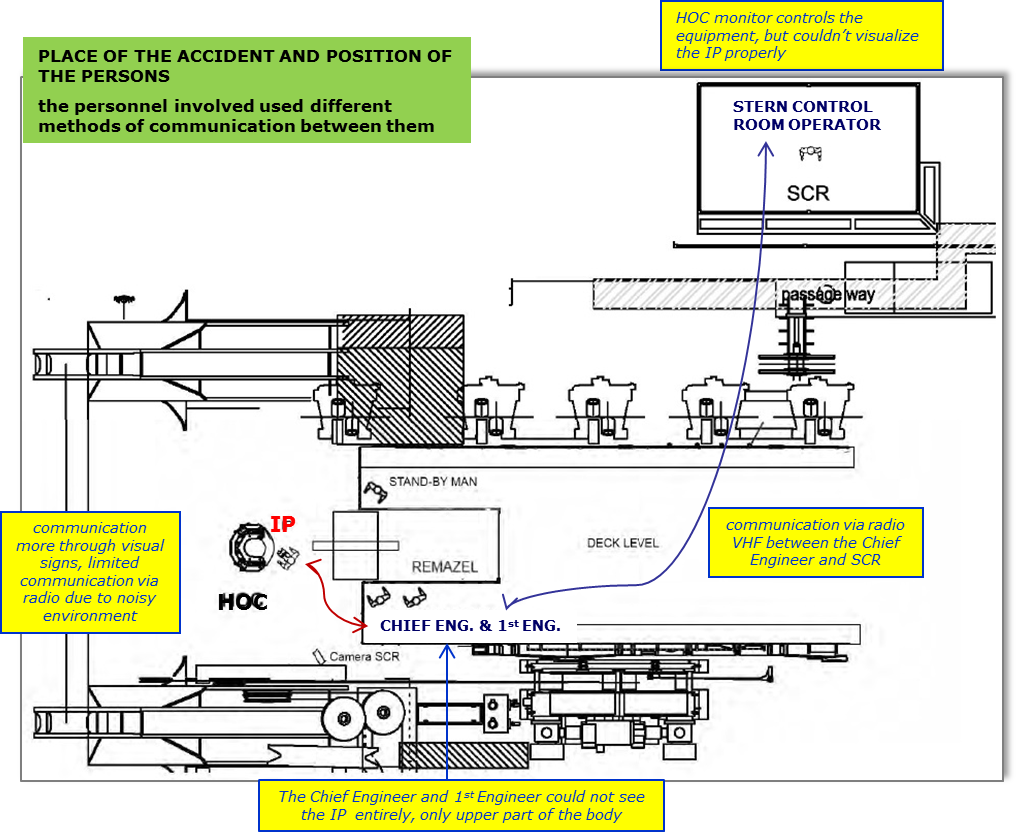
- Improper communication between all persons involved:
- injured person and supervisory team communicated using hand and visual signals and there was no confirmation that the signals were understood as intended
- 1st Engineer and control room operator communicated by radio
- There was no communication between injured person and control room operator;
- The control room operator could see the hang-off clamp, but could not see personnel working nearby;
- There was no evidence of any toolbox talk before the operation to agree on proper communication channels or planning of the operation;
- Whilst a job safety analysis and permit to work had been issued, these did not fully identify the task hazards.
The following corrective actions were taken:
- Improved job safety analysis to ensure adequate identification of all hazards and mitigation measures;
- Improved communication protocols and instituted use of common communications channel between crew and control room.
Safety Event
Published: 9 May 2013
Download: ![]() IMCA SF 07/13
IMCA SF 07/13
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.