Update to SF 11/19: Fatality and multiple injuries – flash fire onboard pipe-lay barge
This Safety Flash comprises an update on the flash fire which occurred onboard a pipe-lay barge earlier in 2019, and includes our members’ findings on the causes of the incident, and lessons learned.
What happened
During pipelaying activities, Injection Moulded Polypropylene (IMPP) equipment used for field joint coating got stuck. Pipelaying activities were stopped and repair operations were started. The crew started to dismantle the machine to investigate the problem. It was discovered that the piston was stuck (i.e. seen tilted from the open flange) inside the accumulator chamber (Figure 1). While trying to pull out the stuck piston using a threaded bar, the heating elements were energized in order to avoid the solidification of the polypropylene contained in the accumulator chamber, and thus to ease the pulling operations.
Whilst at the final stage of extracting the piston, a cloud of flammable vapour and fine polypropylene droplets blew out from the accumulator chamber. The cloud ignited, resulting in a so called “flash-fire” in which fourteen persons were injured. The fire was extinguished by the barge crew.
After medical evacuation, one of the injured crew members subsequently died in hospital.
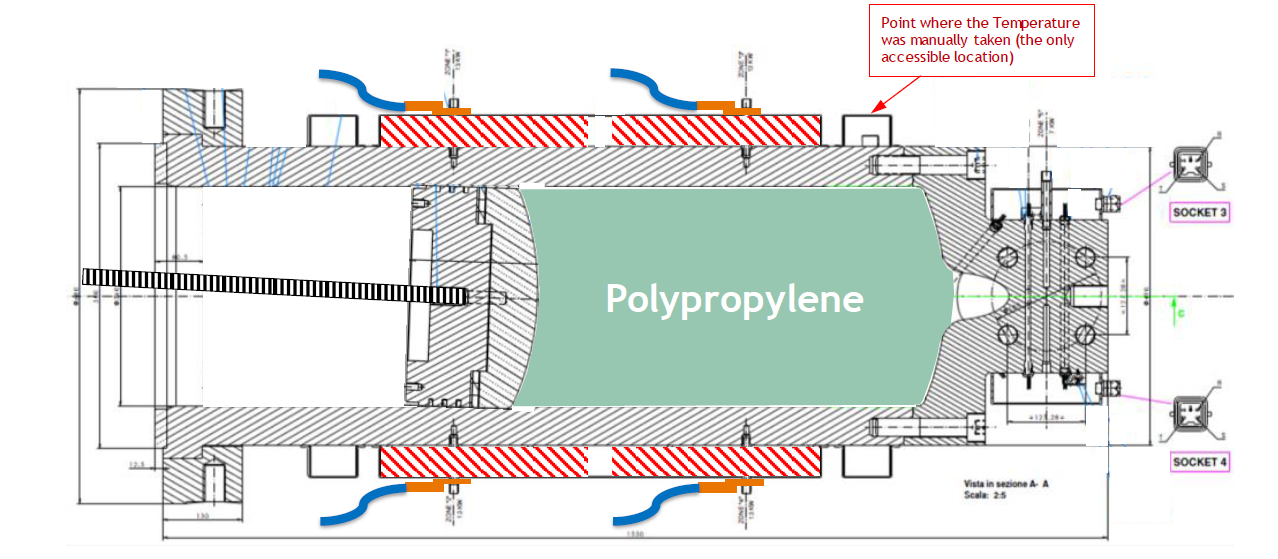
Figure 1 – Known configuration of the accumulator chamber while starting repair activities.
Immediate Actions
- The Company Emergency and Crisis Plan was activated, arranging the necessary support to the barge;
- The fourteen injured persons were evacuated to the local hospital ashore by supply vessel, the planned and foreseen secondary mean of evacuation due to helicopter weather restrictions;
- Dedicated ambulance flights were then arranged to further evacuate the injured persons to specialized hospitals (burns centre);
- The barge was towed alongside and an independent investigation process started.
What went wrong?
The crew connected the IMPP equipment built-in heating system to an external power supply (i.e. replacing the temperature and pressure control system with manual temperature control) to ease the extraction of the melt piston. This resulted in loss of control of the temperature inside the accumulator and, ultimately in overheating the polypropylene accumulated inside (Figure 2).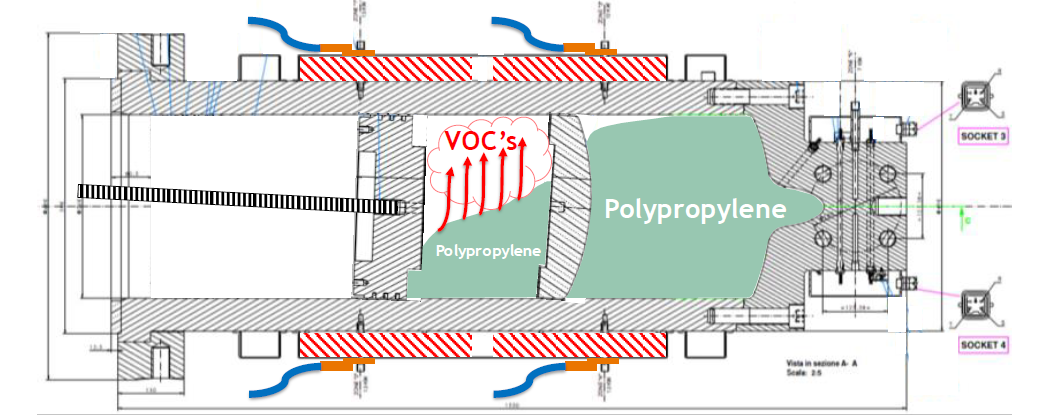
Figure 2 – Real configuration of the accumulator chamber during the repair activities, where the bimetallic piston had split into 2 pieces, causing a partial dam effect and thus an uneven distribution of polypropylene.
The main causes of the accident can be summarised as follows:
- The task of extracting the melt piston was not captured under any procedure nor included in the user manual. It should have been subject to the Management of Change process;
- The Control of Work package did not properly address the need to heat the accumulator;
- The IMPP equipment was regarded as a ‘foreign’ piece of equipment and not something under the accountability of the vessel management team.
- The IMPP equipment has been designed and manufactured by a vendor under the functional specifications provided by the company.
- There were company personnel involved in the design, engineering and construction phases of the IMPP equipment.
- It was not clear where accountability for the equipment lay in terms of repair/maintenance activities.
Lessons Learned
- Custom-made production equipment should be always provided with a comprehensive operation and maintenance manual, including ordinary repair operation and definition of battery limits, beyond which shore approval should be required (MoC process);
- The behaviour of chemicals and fluids processed by the equipment should be fully analysed against undesired deviations from operating conditions. This information should be assessed and reviewed during the relevant safety studies (i.e. HAZOP, FMECA, etc.), as well as part of the operators’ training package.
- For custom-made production equipment, ensure the availability of hand-over report between the supplier/developer (i.e. vendor, engineering, etc. ) and the final owner (i.e. Asset and Operations), including the formal transfer of all documentation (i.e. Manuals, Safety Studies, FAT, SIT, etc.);
- The Control of Work package (i.e. task plan, permit to work, risk assessment, etc.) should always be consistent with the real situation and revised every time a change occurs or inconsistencies are identified.
0
Safety Event
Published: 22 October 2019
Download: ![]() IMCA SF 24/19
IMCA SF 24/19
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.