BSEE: Overhaul Ball falls to deck resulting in High Potential near miss
What happened
The United States Bureau of Safety and Environmental Enforcement (BSEE) has published Safety Alert 460 relating to a dropped object during lifting operations. While conducting crane operations during decommissioning/well abandonment, a 350kg crane “headache ball” fell 8m to deck and landed less than 60cm from one of the riggers.

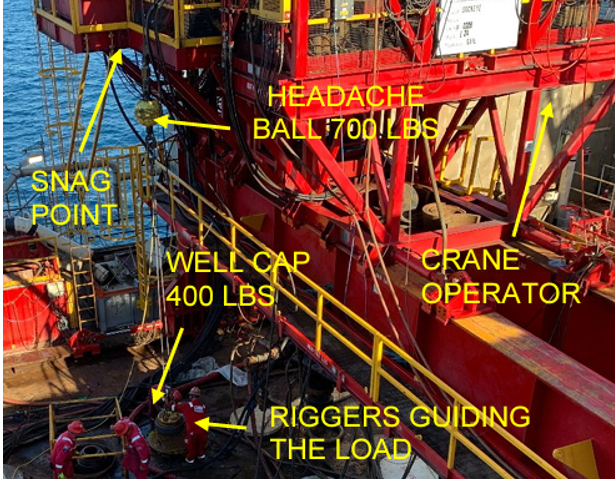
A crane was moving a 200kg (400 lb) well cap when a wedge socket on the auxiliary line snagged on the flange of a C-channel located at the edge of the platform’s rig deck. The lift required running the crane’s auxiliary line within centimetres of the edge of the platform. It was a “blind lift,” directed by a rigger using radio communications. The rigger was standing on the pipe deck and had a clear view of the load, line, pedestal crane, and crane operator. His location put him approximately 9m from the load line.
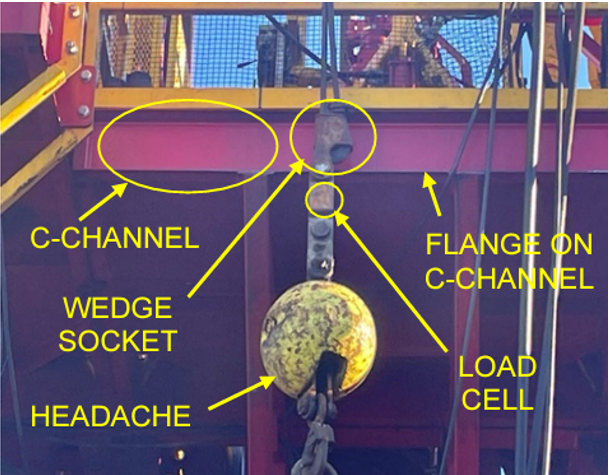
The wedge socket above the headache ball snagged on the C-channel flange that ran across the length of the edge of the deck. This snag temporarily held all the weight of the load and rigging, resulting in a false reading on the auxiliary winch – the load cell sending a weight signal to the operator was below the snagged wedge socket.
The crane operator did not detect that the auxiliary winch was no longer holding the weight of the load. The rigger did not realize that the line had snagged on the C-channel and continued giving directions to keep lowering the load. As the load cell was positioned below the snag, there was no change in the load signal, even though the weight of the load was now being supported by the C-channel and not the auxiliary winch.
The rigger, not seeing any movement, repeated a request to lower the load. Because the crane operator could not see the winch drum behind the crane cab, he did not see that the load was not moving and responded that he was still lowering the load. As the crane operator continued to unwind the auxiliary line at the winch drum, the wedge socket slipped off the flange of the C-channel, releasing the snag. The headache ball fell 8m and hit the deck less than 60cm from one of the riggers guiding the load.
What went wrong?
BSSE identified several contributing factors
- The rigger and crane operator should have noticed the auxiliary winch was no longer detecting the weight of the load;
- The engineered controls (i.e., weight indicator) provided an inaccurate representation to the crane operator of the weight on the winch due to the wedge socket snagging above the load cell;
- The crane operator and rigger failed to recognize something was wrong after repeated requests to lower the load and after receiving the response that the line was being lowered and not seeing any movement in the load position;
- The rigger did not check the path of the auxiliary line for potential snags;
- The work team ought have noticed the potential hazards of working close to the C-channel at the edge of the platform rig, and should have recognized the potential snag points;
- No formal risk assessment was conducted. However, a review of the task was performed.
Lessons and actions
- Ensure a secondary device (e.g., weight indicator, camera) is accessible to detect any slack on the load line;
- Identify all potential rigging contact or snag points and include them in worksite instructions, risk assessments, and toolbox talks – particularly when working close to other equipment or structures;
- Ensure fully agreed, understood and practiced/tested communication between crane driver and rigging crew;
- Ensure a full and thorough lift plan is place before the job is started;
- What would you have done to avoid this situation? Discuss what key controls are in place to remove yourself and your team members from the potential “line of fire”.
Members may wish to refer to:
- Snagged load, a sling snaps, dropped objects: persons injured [a focus on “snagging”]
- Near miss: winch wire snagged and released suddenly [The driller failed to notice that the winch wire had become snagged and continued to…]
- Snagged lift during deck cargo operations (MSF)
Safety Event
Published: 24 July 2023
Download: ![]() IMCA SF 18/23
IMCA SF 18/23
IMCA Safety Flashes
Submit a Report
IMCA Safety Flashes summarise key safety matters and incidents, allowing lessons to be more easily learnt for the benefit of all. The effectiveness of the IMCA Safety Flash system depends on Members sharing information and so avoiding repeat incidents. Please consider adding [email protected] to your internal distribution list for safety alerts or manually submitting information on incidents you consider may be relevant. All information is anonymised or sanitised, as appropriate.
IMCA’s store terms and conditions (https://www.imca-int.com/legal-notices/terms/) apply to all downloads from IMCA’s website, including this document.
IMCA makes every effort to ensure the accuracy and reliability of the data contained in the documents it publishes, but IMCA shall not be liable for any guidance and/or recommendation and/or statement herein contained. The information contained in this document does not fulfil or replace any individual’s or Member's legal, regulatory or other duties or obligations in respect of their operations. Individuals and Members remain solely responsible for the safe, lawful and proper conduct of their operations.